Ready to Build Smarter HealthTech Systems?
Digital transformation in healthcare is happening now. But behind every AI-powered diagnostic tool or predictive model lies something less glamorous but essential: IT infrastructure.
This guide dives deep into the what, why, and how of AI infrastructure in HealthTech, packed with real-world examples, strategic steps, and insider tips to future-proof your systems.
Why Healthtech Needs Purpose-Built AI Infrastructure
AI isn’t a software plugin you download — it’s a living, breathing engine that relies on the right digital environment to function. In HealthTech, that environment must do more than just run — it needs to scale, self-correct, protect, and perform without fail.
Here’s why cloud infrastructure makes all the difference:
Scale on Demand: as models get more sophisticated and datasets grow (think imaging, genomic data, or EHR), your infrastructure must scale elastically, without outages or bottlenecks.
Optimize Costs: streamlining compute resources (GPUs, storage, data transfer) cuts cloud bills and reduces wastage. Efficient architecture pays for itself over time.
Zero Downtime: AI in healthcare must be resilient — no one can afford downtime in the ICU or during patient intake. Fault-tolerant design ensures 24/7 performance.
Speed to Market: agile DevOps, CI/CD pipelines, and containerization accelerate innovation — so your product hits the market faster and evolves in real time.
When the infrastructure isn’t there, even the most powerful AI models can stall. That’s why infrastructure is more than a foundation — it’s the nervous system of your AI product.
Core Components of AI Infrastructure in HealthTech
A high-performing AI infrastructure is a symphony of technologies working in sync.
At Gart, we help orchestrate these layers for maximum harmony.
Layer Components Purpose / Benefits 1. Hardware Layer - GPUs/TPUs: For model training, especially deep learning - CPUs: Ideal for inference in production systems - NVMe Storage: Lightning-fast access to massive datasets Provides computational power and high-speed storage required for AI workloads 2. Software Stack - ML Frameworks: TensorFlow, PyTorch, JAX (custom-fitted for healthcare data) - Data Pipelines: Apache Kafka, Spark (real-time data processing) - Containerization: Docker, Podman (reproducible environments) Builds, trains, and deploys AI models efficiently in robust environments 3. Orchestration & Monitoring - Kubernetes: Orchestrates deployment and scales containers - Prometheus & Grafana: Real-time monitoring and visualisation - CI/CD Pipelines: Jenkins, ArgoCD, GitLab CI (automated deployments) Ensures scalable, resilient, and automated AI operations 4. Security & Governance - RBAC & IAM: Controls data access - Compliance Frameworks: HIPAA, GDPR, SOC2 - Audit Trails & Encryption: Protects data in motion and at rest Guarantees compliance, data privacy, and patient trust 5. Infrastructure as Code (IaC) - Terraform: Deploys secure, version-controlled environments across AWS, Azure, or hybrid clouds Enables rapid, repeatable, and secure infrastructure management
How AI Infrastructure Actually Works
Let’s break down what an AI infrastructure pipeline looks like in action:
Data Ingestion From wearable devices, EHRs, CT scans, and lab results, data flows into your system continuously.
Data Transformation Raw inputs are cleaned, normalized, and structured using tools like Spark or Hadoop.
Model Training Training happens on high-performance GPUs, orchestrated via Kubernetes to manage compute usage.
Model Packaging & Deployment Models are containerized and deployed into real-time production systems using CI/CD pipelines.
Inference Engine Live predictions are served in milliseconds to doctors or backend systems using APIs or edge devices.
Monitoring & Feedback Loop Every prediction is logged, audited, and used to improve models through continuous retraining.
This isn't a static system — it's a loop. The more it runs, the smarter it gets.
Your Blueprint: How to Build AI Infrastructure in HealthTech
Building this isn’t about picking tools randomly — it’s a layered strategy.
Here’s the plan:
Step 1: Define the Use Case
Real-time ICU monitoring?
Radiology image analysis?
Chatbots for triage?
Something else?
Use Case you are trying to solve and hypothesis behind it – must go first!
Define the "why" (and why people pay you, for your solution), which goes before anything else.
Step 2: Scope the Data Requirements
What’s the data volume, velocity, and variety?
Do you need batch processing, streaming, or both?
Step 3: Architect Your Stack
Cloud-native, hybrid, or on-prem?
How will security, logging, and data lineage be handled?
Step 4: Select the Right Tech
Choose tools that your team knows — or partner with experts like Gart Solutions to guide implementation.
Step 5: Enforce Security & Compliance
Don’t treat this as an afterthought. Start with HIPAA-readiness and future-proof your stack.
Step 6: Automate & Iterate
With IaC, build environments with one click. Use telemetry to refine continuously.
What Should Be in Tech Stack for HealthTech Project?
Layer Tech Examples Ingestion & Storage Kafka, Hadoop, Cassandra, S3 Processing & Analytics Spark, Flink ML Frameworks TensorFlow, PyTorch Containerization Docker, Podman Orchestration Kubernetes, Mesos CI/CD & DevOps Jenkins, GitLab CI, ArgoCD Monitoring & Logging Prometheus, Grafana, ELK Security & Compliance IAM, RBAC, encryption, audit logs
And always combine with:
SLA-driven monitoring
MLPerf benchmarking
Cross-functional collaboration
AI Infrastructure Projects in HealthTech: Real-World Use Cases
Across the global health and AI sectors, forward-thinking organizations are building powerful infrastructure to turn AI from theory into impact.
Below is a curated list of real-world projects showcasing how AI-ready infrastructure drives outcomes — and how Gart Solutions can deliver the architecture to support them.
Smart Hospital Systems
Cleveland Clinic
Real-time AI sepsis alerts are built into the EHR system, reducing ICU mortality and time to treatment.
The clinic requires GPU-enabled inference, EHR access via FHIR APIs, and HIPAA-compliant pipelines.
Oulu University Hospital (Finland):
AI for Operational Efficiency
Memorial Regional Hospital (USA):
AI-based bed management system predicted availability with > 90% accuracy, saving millions and shortening ED wait times.
The hospital requires the ingestion of scheduling and patient flow data, and Gart can help utilize AI for operational efficiency of the hospital.
Midwest Health System:
Workforce optimization AI, orchestrated via Kubernetes, saving $8.7M/year.
Ingested shift logs, patient acuity, and census data for predictive modeling.
Infrastructure focus: Secure data lakes, predictive pipelines, and automated deployment frameworks — exactly what Gart delivers through IaC and MLOps.
Research & Federated AI
Mayo Clinic Platform
Federated AI across multiple hospitals, sharing model weights, not data — for privacy-preserving research.
Owkin
Distributed AI training for drug discovery using federated learning infrastructure.
Gart value: Expertise in secure multi-cloud orchestration, encrypted communication, model governance, and federated training setups.
Radiology & Imaging AI
Aidoc Medical
Always-on AI running at radiology workstations and backend servers — automatically flags emergencies (e.g., stroke, hemorrhage) across 1,500+ hospitals.
Portal Telemedicina (Brazil)
Google Cloud-powered AI reading chest x-rays in rural clinics with edge-based diagnostics and cloud-based monitoring.
What’s required: High-speed NVMe storage, container orchestration (K8s), real-time inference APIs, model drift monitoring — all supported by Gart’s infrastructure design.
National & Cross‑Institutional Research Networks
Swiss Personalized Health Network (SPHN)
Nationally governed data architecture for AI-driven precision medicine.
Infrastructure insight: These use cases need interoperable APIs (FHIR, HL7), robust governance frameworks, secure compute clusters, and cloud-native elasticity, and Gart can deliver that.
Summary Table: AI Use Cases vs Infrastructure Needs
Project Type Infrastructure Components Required Smart Hospitals 5G, IoT, Edge compute, EHR APIs Operational AI Data ingestion, analytics pipelines, orchestration Federated AI Secure model sharing, distributed training, encrypted comms Radiology/Diagnostics GPU clusters, NVMe storage, real-time inference
Who’s Behind the Curtain? Common Roles in AI Infrastructure
Role Responsibility AI Infrastructure Engineer Designs and scales compute/storage pipelines Data Scientist Develops and validates AI models DevOps Engineer Builds CI/CD, containerization, IaC ML Engineer Bridges models into production systems Compliance Officer Ensures HIPAA, GDPR, SOC2 adherence
Gart helps you assemble this team or supplements your internal one, based on project phase and complexity.
Let Gart Solutions Lead the Way
With deep expertise in cloud architecture, compliance automation, and AI enablement, Gart Solutions provides:
- Turnkey AI infrastructure for health startups and enterprises - Compliance-ready deployment stacks via Terraform and IaC - Real-time observability and SLA-backed performance - Support for EHR integration (Epic, Athena, Cerner) using FHIR APIs - Optional edge-AI and federated learning architectures
We blend the speed and modern practices with the depth, security, and healthcare domain expertise you won’t find in generalist vendors.
Start Building — The Right Way
Infrastructure isn’t the sexiest part of AI, but it’s the most important.
Done wrong, it leads to slow deployments, security nightmares, and underperforming models. Done right, it’s your secret weapon.
Let Gart Solutions help you build the AI infrastructure that powers breakthrough patient care, real-time diagnostics, and compliant innovation at scale.
Get a sample of IT Audit
Sign up now
Get on email
Loading...
Thank you!
You have successfully joined our subscriber list.

What is Digital Transformation in Healthcare?
Digital transformation in healthcare is no longer a future trend — it is the operational baseline for organizations that want to survive and lead in 2026.
Digital transformation in healthcare refers to the systematic integration of digital technologies — AI, cloud infrastructure, IoT, telemedicine, electronic health records (EHR), robotics, and advanced analytics — into every dimension of healthcare delivery, management, and operations.
It goes far beyond swapping paper for screens. A genuine digital transformation rethinks how hospitals, clinics, labs, and insurers create value for patients and how they collaborate across the entire care continuum.
Simple definition: Digital transformation in healthcare means using technology to fundamentally improve how care is delivered, experienced, and paid for — not just digitizing existing processes, but redesigning them from the ground up.
This guide breaks down 10 real implementation cases, the most common challenges, measurable benefits, and a practical roadmap for healthcare leaders.
Why Is It Gaining Momentum Now?
Several converging forces accelerated healthcare digitization well beyond the COVID-19 period:
Rising patient expectations:Patients compare healthcare to their experience with Amazon or Netflix and demand convenience, personalization, and instant access to their data.
Technology maturity:AI, large language models, and IoT devices reached production-grade reliability that makes large-scale healthcare deployment viable.
Financial pressure:Hospital margins compressed significantly post-pandemic. Automation and digital workflows are now a profitability lever, not a luxury.
Regulatory mandates:Governments from the US to the EU now require interoperable digital health records, telemedicine reimbursement frameworks, and mandatory data security standards.
Workforce shortages:With over 10 million unfilled healthcare roles globally projected by 2030 (WHO), automation and AI-assisted care are becoming a workforce strategy.
A Statista report projects the global digital healthcare market to reach $504.4 billion by 2025, underscoring how essential digital transformation has become for competitive and efficient healthcare delivery.
88% of healthcare technology leaders prioritize improving the patient experience in their investments (according to a Deloitte survey)
This shift underscores the necessity for healthcare professionals, including doctors, nurses, and administrative staff, to stay abreast of ongoing digital advancements.
Key Drivers of Digital Transformation in Healthcare (2026)
Artificial Intelligence
AI has crossed from experimental to mission-critical in healthcare. Today it powers:
Automated clinical documentation that reduces physician burnout
Diagnostic imaging analysis for radiology, pathology, and ophthalmology with accuracy matching or exceeding specialists
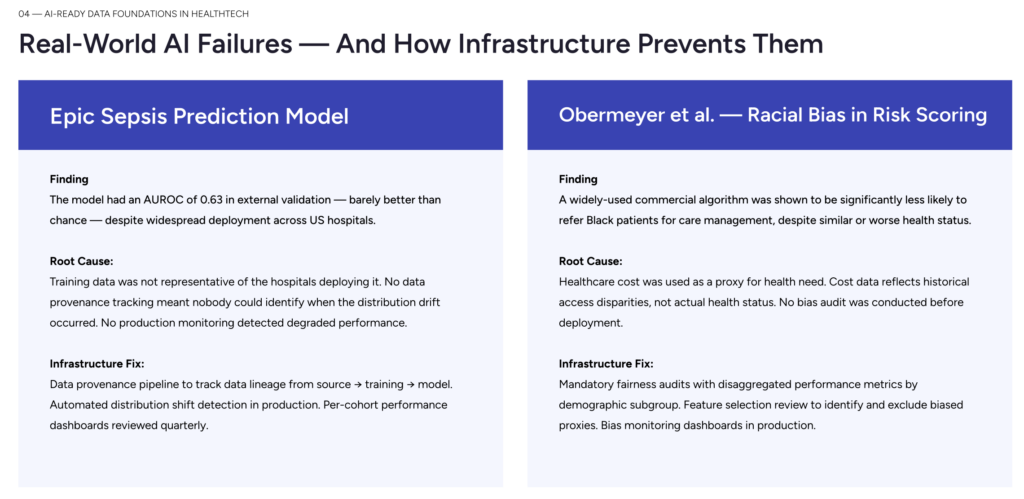
Predictive risk scoring for sepsis, cardiac events, and readmission prevention
AI-powered triage chatbots that handle over 30% of patient inquiries without human escalation
Drug discovery acceleration through molecular simulation (reducing timelines from years to months)
Google DeepMind's AlphaFold resolved a 50-year protein-folding problem, and its healthcare applications now inform drug design globally — a concrete proof point that AI delivers transformative, not incremental, value.
Internet of Things (IoT) in Healthcare
The number of connected medical devices globally exceeded 500 million in 2025. These devices enable:
Continuous remote patient monitoring for chronic conditions, reducing hospital admissions by up to 38%
Smart hospital infrastructure (asset tracking, bed management, HVAC optimization)
Wearable biosensors detecting arrhythmias, hypoglycemia, and medication adherence in real time
Cloud Infrastructure
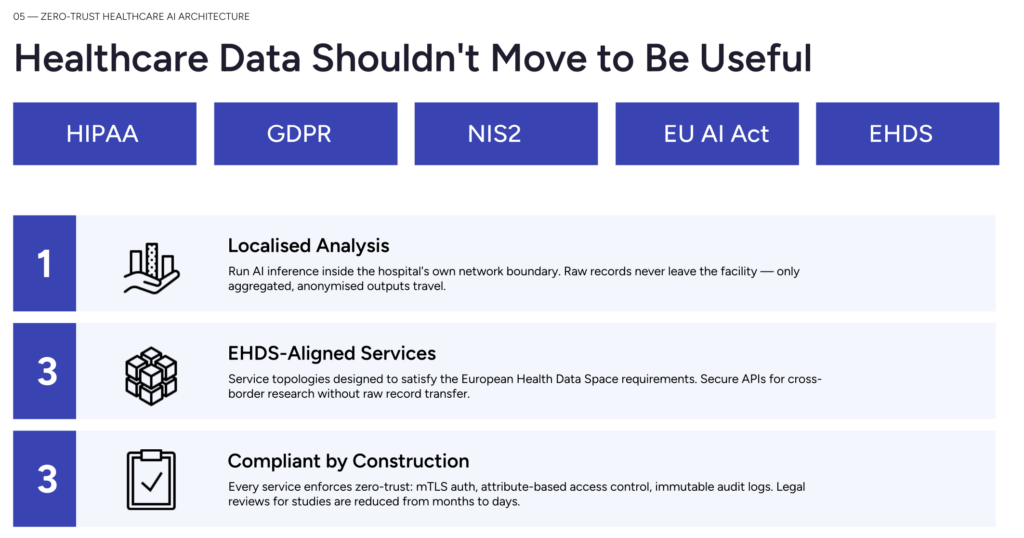
Modern healthcare digital transformation runs on HIPAA-compliant cloud platforms. Cloud enables scalable data storage, real-time analytics, disaster recovery, and the computational power required for AI workloads — without the capital cost of on-premise data centers.
Robotics and Automation
Beyond the well-known da Vinci Surgical System, robotics now extends to hospital logistics (automated medication dispensing, supply chain robots), rehabilitation (exoskeletons), and AI-assisted clinical decision support that automates protocol-driven care decisions.
Measurable Benefits of Digital Transformation in Healthcare
The audit of this content flagged that generic benefit lists are insufficient. Below is a structured view with real benchmarks:
Benefit AreaWhat It MeansReal-World MetricCost ReductionAutomating administrative tasks (scheduling, billing, coding) and optimizing infrastructure15–30% reduction in IT operational costs; up to 40% reduction in administrative overheadWorkflow OptimizationAI-assisted triage, digital care pathways, and automated alerts reduce manual bottlenecksDeployment time reduced from days to hours (CI/CD implementation cases)Patient OutcomesEarlier diagnosis, personalized treatment plans, and reduced preventable readmissions38% reduction in hospital readmissions with remote monitoring programsInteroperabilityUnified patient data accessible across departments and care settingsReduced duplicate testing, faster diagnosis cyclesRevenue CycleAutomated claims processing, error reduction, and faster reimbursementDenial rates drop significantly with AI-powered coding assistanceSecurity & ComplianceContinuous monitoring, encryption, and automated compliance controlsProactive detection of incidents before they escalate to breachesMeasurable Benefits of Digital Transformation in Healthcare
Key Takeaway
The ROI of digital transformation in healthcare is not just financial.
Hospitals that have successfully digitized report improved staff satisfaction, higher patient NPS scores, and significantly faster time-to-care
— outcomes that reinforce each other in a virtuous cycle.
Challenges to Healthcare Digital Transformation (and How to Overcome Them)
🔒
Data Privacy & Security
Healthcare data is 10× more valuable than financial data on the dark web, making it the top target for ransomware. HIPAA, GDPR, and ISO 27799 compliance is non-negotiable.
🏗️
Legacy System Integration
Most healthcare organizations run on 10–20 year old systems. Integrating modern platforms with these via HL7 FHIR standards requires careful architecture planning.
👥
Resistance to Change
Clinical staff distrust technology that disrupts established workflows. Change management, co-design with clinicians, and phased rollout dramatically increase adoption rates.
🎓
Skills Gaps
Digital literacy varies widely across healthcare workforces. Continuous training programs and UX-first technology design are the twin levers for closing this gap.
💰
Cost of Implementation
Enterprise digital transformation has high upfront costs. Cloud-first and phased approaches reduce capital risk while delivering measurable ROI within 12–18 months.
🔄
Interoperability Gaps
Data silos between EHR, labs, and payers prevent unified views. HL7 FHIR R4 and modern API-first architecture are the industry's emerging answer.
10 Real-World Cases of Digital Transformation in Healthcare
1
Infrastructure Optimization & Data Management in Healthcare
Challenge
A health tech company operated on outdated, non-scalable infrastructure with frequent downtimes that directly impacted patient care operations and data availability.
Solution
Gart Solutions implemented a comprehensive infrastructure modernization: legacy system migration to cloud, HIPAA-compliant secure data management pipelines, and dynamic auto-scaling.
Impact
Eliminated critical downtimes, reduced data access latency, and achieved full HIPAA compliance — enabling the organization to scale operations without infrastructure risk.
Read the full case study →
2
CI/CD Pipelines for an E-Health Platform
Challenge
An e-health platform suffered from slow, error-prone manual deployments that delayed feature releases and introduced instability in a compliance-sensitive environment.
Solution
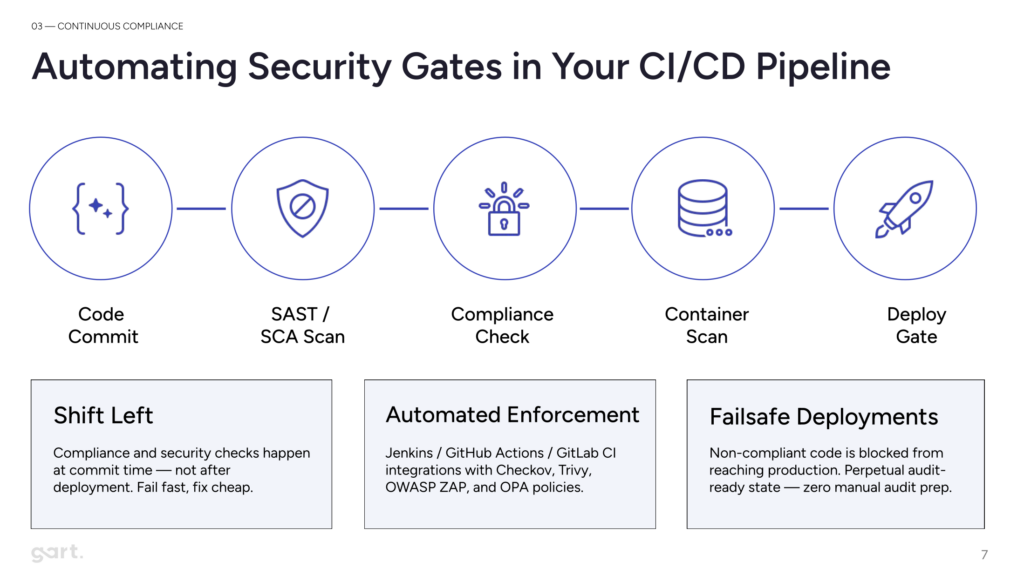
Automated CI/CD pipelines with Kubernetes orchestration, integrated compliance checks, and real-time monitoring with automated rollback capabilities.
Impact
Deployment time dropped from days to hours. Human error rates fell significantly. Feature velocity increased, enabling the platform to respond faster to clinical user needs.
View case study →
3
Electronic Medical Records (EMR) for a Government E-Health Platform
Challenge
A government E-Health initiative required a compliant, secure EMR platform with strict HIPAA and GDPR requirements, deployed on local cloud infrastructure.
Solution
Gart deployed on-premises CI/CD pipelines using GiGa Cloud hardware with VMware ESXi, Terraform, and data-masking techniques for non-production environments.
Impact
Delivered a fully compliant, secure EMR system enabling the government platform to serve thousands of patients while passing all regulatory audits.
4
Healthcare SaaS Migration: AWS to Azure with PHI Compliance
Challenge
A high-growth healthcare SaaS company needed to revamp CI/CD pipelines for .NET and Node.js environments and migrate from AWS to Azure without disrupting PHI access compliance.
Solution
Gart implemented Terraform infrastructure-as-code, rebuilt CI/CD pipelines for both stacks, and orchestrated a zero-downtime cloud migration with compliance maintained throughout.
Impact
Seamless migration with full PHI access compliance maintained. Improved infrastructure cost efficiency and development velocity post-migration.
5
HIPAA Migration: HealthCareBlocks to AWS (Ruby on Rails)
Challenge
A Ruby on Rails healthcare application needed migration from HealthCareBlocks to Amazon AWS with strict HIPAA compliance requirements and zero tolerance for data integrity risk.
Solution
Gart led a meticulous migration with continuous HIPAA compliance validation at every stage, encryption in transit and at rest, and a phased cutover to eliminate downtime risk.
Impact
Full migration completed without compliance incidents. Application performance improved on AWS infrastructure with better scalability for future growth.
6
ISO 27001 Compliance & Cloud Migration (Spiral Technology)
Challenge
Spiral Technology faced dual challenges: achieving ISO 27001 certification and migrating to cloud simultaneously, with data security as the primary constraint.
Solution
Gart provided end-to-end ISO 27001 implementation guidance, risk assessment frameworks, and a detailed cloud migration plan with advanced encryption and monitoring.
Impact
ISO 27001 certification achieved. Continuous monitoring established post-migration to maintain compliance and detect emerging threats in real time.
7
Google DeepMind Health — AI Diagnostics for Ophthalmology
Challenge
Ophthalmology screening capacity globally is constrained by specialist availability, causing diagnosis delays for conditions like diabetic retinopathy and age-related macular degeneration.
Solution
DeepMind Health developed an AI system trained on retinal scans that can detect over 50 eye conditions with accuracy matching or exceeding specialist ophthalmologists.
Impact
Deployed in major hospital systems, the AI enables rapid first-line screening, routing only complex cases to specialists — dramatically increasing diagnostic throughput.
8
Telehealth at Scale — Pandemic Response & Beyond
Challenge
The COVID-19 pandemic created overnight demand for remote consultation infrastructure that most healthcare systems were not equipped to deliver at scale.
Solution
Health systems globally rapidly deployed cloud-based telehealth platforms, integrated with EHR systems, enabling video consultations, e-prescriptions, and remote monitoring.
Impact
Telehealth usage surged over 154% vs pre-pandemic levels. Beyond the crisis, a permanent behavioral shift: patients now expect remote access as a standard offering.
9
IoT-Enabled Remote Patient Monitoring for Chronic Disease
Challenge
Patients with chronic conditions like heart failure and COPD represent a disproportionate share of hospital readmissions, driven by delayed detection of deteriorating vitals.
Solution
IoT remote monitoring programs deploy connected biosensors that transmit real-time vitals to clinical dashboards, triggering automated alerts when thresholds are crossed.
Impact
Hospital systems report up to 38% reduction in 30-day readmission rates — one of the highest-ROI interventions in value-based care.
10
Robotic Process Automation (RPA) in Healthcare Administration
Challenge
Healthcare administrative staff spend up to 34% of their time on repetitive manual tasks: prior authorizations, claims processing, and scheduling — tasks prone to error and burnout.
Solution
RPA bots handle end-to-end administrative workflows — pulling patient data, filling forms, submitting claims, and triggering exceptions for human review only when needed.
Impact
Organizations report 40–70% reduction in administrative processing time and reallocation of staff capacity to higher-value clinical support work.
How Digital Transformation Enhances Patient Experience
Telehealth and Remote Consultations
The telehealth revolution is permanent. Beyond the pandemic-era necessity, patients now actively choose virtual care for its convenience. Modern telehealth platforms enable:
Real-time video consultations with prescriptions delivered to pharmacy within minutes
Telepsychiatry for mental health access in underserved regions
Continuous remote management of diabetes, hypertension, and cardiac conditions
Second-opinion consultations with specialists regardless of geography
Personalized Medicine and AI Diagnostics
Digital transformation enables care that was genuinely impossible a decade ago. AI-assisted diagnostics analyze radiology images, ECGs, and genomic data to detect diseases at stages where intervention has the highest impact. IBM Watson Health, for example, analyzes thousands of patient records to surface treatment recommendations that clinicians may not have considered.
Predictive analytics now enable proactive rather than reactive care — identifying patients at elevated risk for sepsis, cardiac events, or 30-day readmission before deterioration begins, enabling earlier, cheaper, and more effective interventions.
Patient Data Security as a Patient Experience Issue
Patients increasingly understand that data security is not just a compliance issue — it is a trust issue. Healthcare organizations that demonstrate strong cybersecurity practices, transparent data use policies, and prompt breach response build significantly higher patient loyalty and satisfaction.
Step-by-Step Digital Transformation Roadmap for Healthcare Organizations
Phase 1
Months 1–2
Assessment & Strategy
Conduct an IT infrastructure audit to map current systems, identify compliance gaps, cost inefficiencies, and security exposures. Define transformation goals aligned to clinical and business outcomes.
Phase 2
Months 2–4
Foundation & Security
Establish cloud infrastructure with HIPAA-compliant architecture. Implement IAM, encryption, MFA, and continuous monitoring from day one. This foundation is what everything else builds on.
Phase 3
Months 4–9
Core System Modernization
Migrate priority workloads to cloud. Integrate EHR systems with modern APIs. Deploy CI/CD pipelines for healthcare applications. Begin HL7 FHIR implementation for interoperability.
Phase 4
Months 6–12
Digital Care Enablement
Roll out telehealth platforms, patient portals, and mobile access. Deploy IoT remote monitoring for chronic disease populations. Introduce AI-assisted documentation and triage tools.
Phase 5
Months 9–18
Analytics & AI
Build a unified data platform. Implement predictive analytics for readmission risk, staffing optimization, and supply chain management. Introduce AI diagnostics for clinical workflows.
Phase 6
Ongoing
Continuous Improvement & Scale
Establish KPIs and measure outcomes quarterly. Expand successful pilots across the organization. Maintain compliance posture through regular IT audits and staff training.
Lessons from Failed Healthcare Digital Transformation Projects
Analyzing transformations that underdelivered reveals consistent failure patterns that are entirely preventable:
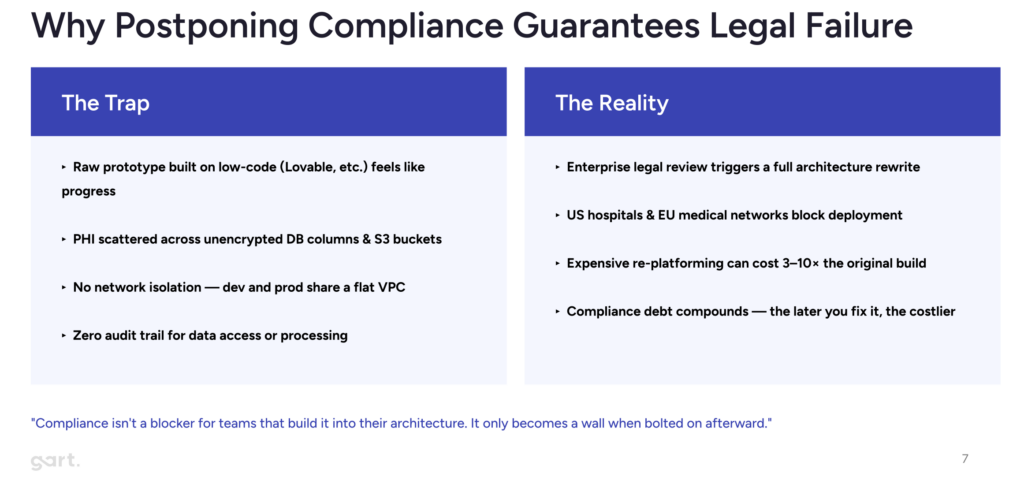
Failure PatternWhat Goes WrongPreventionTechnology-first thinkingDeploying tools without redesigning workflows. Staff work around the technology, defeating its purpose.Start with patient/clinical outcomes. Technology serves the workflow redesign.Big Bang implementationsAttempting full-system replacement in a single cutover event creates catastrophic risk in healthcare.Phased rollout with parallel systems during transition. Pilot → expand.Security bolted on lateCompliance and security added after build creates architectural debt that is expensive and risky to remediate.Security-by-design from the first line of architecture. HIPAA compliance as a design requirement.Underestimating change managementClinical staff resistance kills adoption rates. The best system unused is worthless.Clinicians co-design the solution. Change management and training investment matches technology investment.No clear ownershipTransformation projects without a clinical champion and executive sponsor drift, stall, or get abandoned.Assign a dedicated transformation leader with cross-functional authority and clinical credibility.Lessons from Failed Healthcare Digital Transformation Projects
Regulatory Frameworks Driving Healthcare Digital Transformation
Digital transformation in healthcare does not happen in a regulatory vacuum. Compliance requirements actively shape architecture decisions, vendor selection, and deployment timelines:
FrameworkScopeImpact on Digital TransformationHIPAAUS — Protected Health Information (PHI)Mandates encryption, access controls, audit trails, and breach notification. Shapes all cloud architecture decisions.GDPREU — All personal data including health recordsRequires data minimization, consent management, and right to erasure. Affects global platforms serving EU patients.HITECH ActUS — Electronic Health RecordsIncentivizes meaningful use of EHR technology. HIPAA-compliant apps are considered HITECH compliant.ISO 27001Global — Information Security ManagementGold standard for security governance. Required by many enterprise healthcare clients as vendor qualification.HL7 FHIRGlobal — Interoperability StandardEnables data exchange between different healthcare systems. Increasingly mandated by US CMS for payers.Regulatory Frameworks Driving Healthcare Digital Transformation
Gart Solutions · Healthcare IT Services
Struggling with Your Healthcare Digital Transformation?
Gart Solutions has helped health tech companies navigate infrastructure modernization, HIPAA compliance, cloud migration, and DevOps transformation. We deliver quick wins from day one.
☁️
Cloud Migration
AWS, Azure, GCP — HIPAA-compliant by design
⚙️
DevOps & CI/CD
Automate deployments & reduce clinical downtime
🔍
IT Audit & Compliance
Infrastructure audits, HIPAA, ISO 27001 readiness
🏗️
Infrastructure Mgmt
Managed services, SRE, monitoring & reliability
👔
Fractional CTO
Strategic tech leadership for scaling companies
🔄
Transformation
End-to-end strategy & execution for IT
Get a Free Consultation →
See our healthcare work
★ 4.9 rating · 15+ verified reviews on Clutch · Trusted by health tech companies globally
Conclusion
Healthcare organizations understand that digital transformation is crucial for enhancing healthcare services and strengthening patient relationships. Beyond technology investments, this transformation necessitates a shift in organizational culture and employee engagement, requiring enterprise-wide involvement.
Leading health organizations are adopting six key strategies to advance digitally:
Establish digital leadership and governance aligned with business strategies.
Cultivate a digital culture supported by leadership at all organizational levels.
Develop next-generation talent with a focus on workforce quality and quantity.
Integrate cybersecurity at all stages for robust risk management.
Emphasize flexibility and scalability to adapt to evolving technologies.
Implement measurable, accountable KPIs to track the success of digital initiatives.
Successfully navigating digital transformation in healthcare requires expertise and a business-first approach of IT Consulting.
Gart Solutions can guide healthcare providers through the process of Digital Transformation, accelerating the adoption of digital healthcare technologies and improvement of patient outcomes.
Contact Gart today to learn more about how we can help you solve the challenges of digital transformation in healthcare.
Struggling with digital transformation for your healthcare project? Get expert guidance and IT Consultancy for your project free of charge. “Quick wins” – guaranteed. Contact Us.

AI and machine learning are revolutionizing healthcare, especially in the realm of medical devices, bringing in new ways to diagnose and treat patients. But with this fast-paced innovation comes the tricky task of regulating technology that’s constantly evolving.
Agencies like the FDA in the U.S. and regulatory bodies in Europe are working to keep up, finding ways to make sure these high-tech tools are safe, reliable, and effective. By creating flexible guidelines, building collaborative partnerships, and focusing on real-world monitoring, regulators are adapting to the unique challenges of AI-driven healthcare — aiming to support innovation while keeping patient safety front and center.
Differences in Regulatory Approaches to AI in Healthcare: US vs. Europe
1. Regulatory Structure and Oversight
United States: In the U.S., the Food and Drug Administration (FDA) is the main body overseeing AI in medical devices. It operates under a centralized system with clear processes for classifying devices, assessing risks, and approving them. The FDA’s Digital Health Center of Excellence focuses on AI and machine learning (ML) in healthcare, offering resources and guidance for developers. The FDA itself reviews medical AI devices to make sure they’re safe and effective.
Europe: The European Union (EU) and the United Kingdom (UK) follow a more decentralized system, using third-party certifying bodies for conformity assessments instead of direct government oversight. The EU’s regulatory framework is developed by the European Commission, aiming to create consistent regulations across member states for a smooth internal market. In the UK, the Medicines and Healthcare products Regulatory Agency (MHRA) works with the Department of Health to oversee AI in healthcare.
"Unlike in America, we don’t really have a single agency overseeing medical devices development in Europe... The European Commission drives the policy, aiming for harmonization across member states to support a single market."
Lincoln Tsang, a UK-based legal expert
2. Risk-Based Frameworks for Classification
US FDA: The FDA categorizes AI-based medical devices by their risk level and intended use, with a focus on potential patient impact. Lower-risk devices, like general wellness apps, face minimal oversight, while higher-risk tools, particularly those that influence clinical decisions, go through strict evaluation. The FDA’s guidance highlights functionality, deployment context, and patient safety as key factors in deciding the risk level and regulatory needs.
European and UK Standards: Similar to the FDA, regulators in Europe and the UK classify devices based on functionality, intended use, and patient impact. Both the EU and UK use a risk-based approach to assess whether AI software qualifies as a medical device, examining the potential harm and healthcare role of the device. Unlike the FDA’s centralized model, the EU uses third-party bodies for assessments, adding industry involvement to the review process.
3. Approval Pathways and Compliance Assistance
The FDA offers several resources to help developers, including guidance documents, informal consultations, and a Digital Health Policy Navigator to clarify regulatory requirements. A key tool is the Predetermined Change Control Plan (PCCP), which lets developers update AI models without resubmitting for approval, as long as updates follow pre-approved guidelines.
The EU and UK support emerging tech through policy papers and adaptable guidelines. While EU regulators are considering adaptive AI-specific regulation, they currently use general guidance rather than structured pathways like the FDA’s PCCP. Both regions prioritize flexibility, updating guidelines and consulting with industry to keep up with rapid tech advancements in AI and digital health.
"We understand the impact this has on companies, particularly for smaller companies and startups, which we see a lot of in the digital health space. Predictability in regulation is crucial."
Sonja Fulmer, Deputy Director, Digital Health Center of Excellence
4. International Harmonization Efforts
Recognizing the global reach of AI, the FDA, Health Canada, and the UK’s MHRA collaborate to align standards and practices. This teamwork simplifies the approval process for companies across borders. Through groups like the International Medical Device Regulators Forum (IMDRF), these agencies work on creating standards that support global interoperability, safety, and clarity. The IMDRF also offers guidance on issues like machine learning practices, promoting a unified regulatory approach worldwide.
Third-Party Compliance Audits for Healthcare Startups
Third-party compliance audits are key for healthcare startups to ensure their products meet regulatory standards before hitting the market. Companies like Gart Solutions offer specialized compliance audits and consulting services to help startups align with the rules set by bodies like the FDA in the U.S. and certification organizations in the EU.
These third-party services support startups by helping them:
Assess Regulatory ReadinessThrough preliminary audits and gap assessments, firms like Gart Solutions help startups identify their current compliance status and highlight areas needing improvement.
Prepare for Formal CertificationBy simulating official audit conditions, third-party firms enable startups to address potential issues in advance of formal evaluations by agencies like the FDA or European certifying bodies.
Monitor Ongoing ComplianceSince regulations, particularly around adaptive AI, are constantly evolving, third-party auditors often conduct periodic reviews to ensure products stay compliant. For AI-enabled devices, these audits can also include checks on algorithmic fairness, data quality, and post-market performance.
Benefits of Compliance Audits for Startups
Partnering with third-party compliance firms offers several advantages:
Cost Savings: Catching compliance issues early can prevent expensive delays and rework during regulatory approval.
Streamlined Approvals: A thorough pre-audit can smooth the formal certification process, reducing friction with regulatory bodies.
Increased Trust and Transparency: Third-party audits show a startup’s dedication to safety and transparency, boosting stakeholder and consumer confidence.
In regions like the EU, where third-party assessments are a regulatory standard, companies like Gart Solutions help fill the gap for startups that may not have in-house compliance expertise. This support is especially valuable for AI-driven healthcare startups, where standards are both strict and rapidly changing.
Get a sample of IT Audit
Sign up now
Get on email
Loading...
Thank you!
You have successfully joined our subscriber list.
Why Postmarket Surveillance Matters
Postmarket surveillance plays a vital role in regulating AI in medical devices. For high-stakes uses like sepsis detection tools, the FDA requires a monitoring plan to track real-world performance, ensuring devices remain safe and effective across diverse patient populations. This process means manufacturers need to keep an eye on model bias, data quality, and overall device performance in everyday clinical settings. By actively managing these factors, postmarket surveillance helps reduce risks from data issues or model bias, supporting consistent, reliable performance over time.
Trends and the Future of Regulation
With AI becoming a bigger part of healthcare, regulators are likely to move toward more flexible, adaptive policies. Emerging challenges, like continuous-learning AI algorithms, are pushing agencies to rethink how they manage the entire lifecycle of these technologies. Quality assurance, postmarket surveillance, and adaptable regulations are all set to play a larger role as AI advances.
The FDA is working on guidelines for adaptive AI, expected to be released soon, which will help developers as they build continuously learning algorithms. Meanwhile, regulatory bodies in the UK and EU are exploring similar frameworks suited to their own standards, promoting international alignment and consistency.
Conclusion
The regulatory landscape for AI in healthcare is advancing rapidly to keep pace with technological developments. With their risk-based frameworks, both the FDA and European regulators are focused on ensuring the safety and efficacy of AI-enabled medical devices while supporting innovation. Through resources like the Digital Health Center of Excellence and international harmonization initiatives, agencies are setting the stage for a future where AI can safely and effectively transform healthcare, with robust postmarket surveillance and flexible change management strategies forming the backbone of this evolving regulatory framework.